 De standard-of-care behandeling voor patiënten
met niet-kleincellig longcarcinoom zonder targetable moleculaire veranderingen
is immuuntherapie met anti-PD-(L)1 checkpointremmers met of zonder platina-gebaseerde
doublet chemotherapie. Resistentie tegen immuuncheckpointremming is echter niet
ongebruikelijk. De multinationale fase 2 umbrella
trial HUDSON heeft gerichte therapieën tegen mogelijke resistentiemechanismen
geëvalueerd. Prof. John Heymach (MD Anderson Cancer Center, Houston TX) en
collega’s publiceren de studie in Nature Medicine.1
De standard-of-care behandeling voor patiënten
met niet-kleincellig longcarcinoom zonder targetable moleculaire veranderingen
is immuuntherapie met anti-PD-(L)1 checkpointremmers met of zonder platina-gebaseerde
doublet chemotherapie. Resistentie tegen immuuncheckpointremming is echter niet
ongebruikelijk. De multinationale fase 2 umbrella
trial HUDSON heeft gerichte therapieën tegen mogelijke resistentiemechanismen
geëvalueerd. Prof. John Heymach (MD Anderson Cancer Center, Houston TX) en
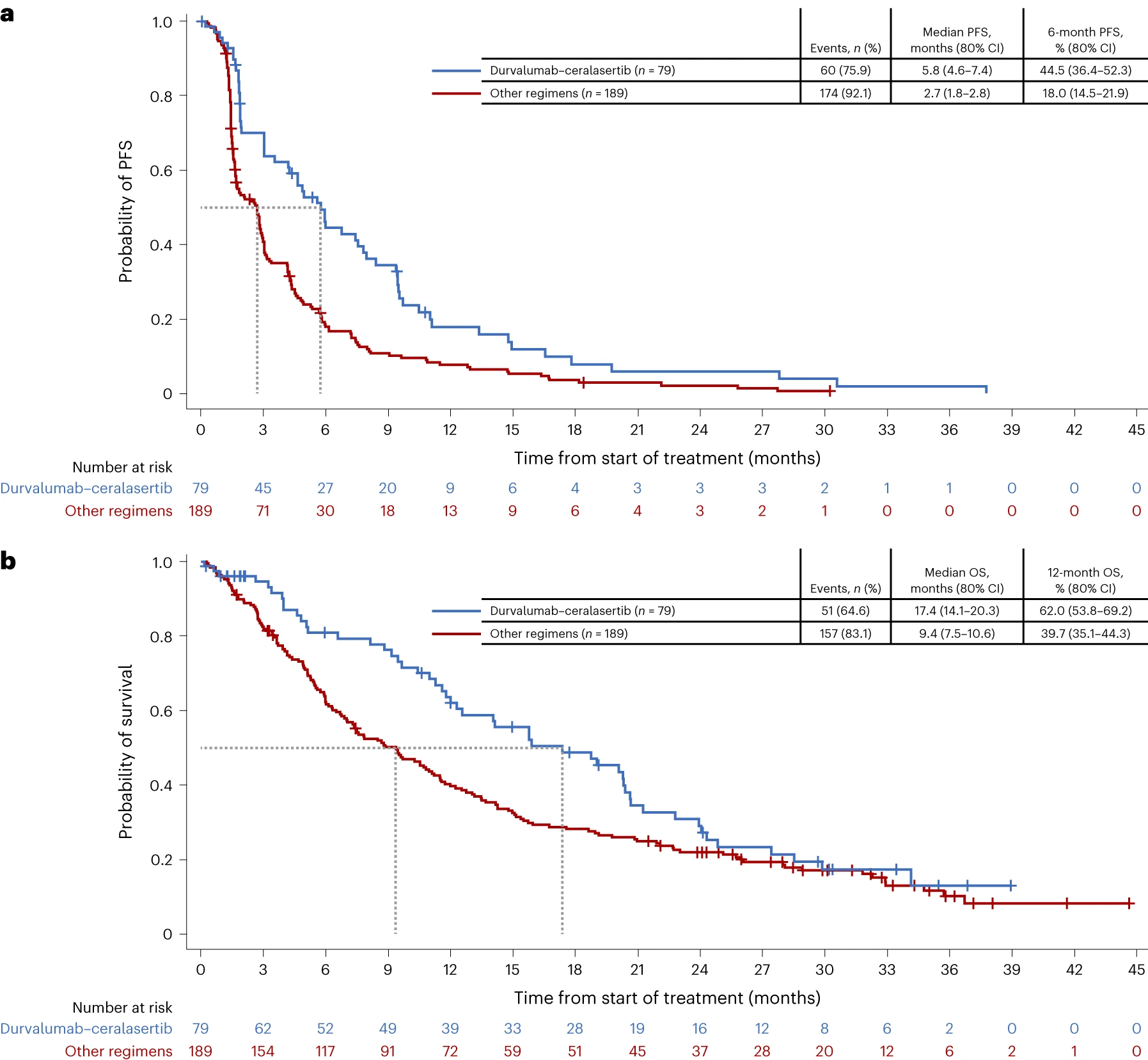
collega’s publiceren de studie in Nature Medicine.1De studie includeerde 268 patiënten met gevorderd niet-kleincellig longcarcinoom na falen van anti-PD-(L)1 therapie en platina-doublet therapie. De patiënten kregen durvalumab in combinatie met één van vier tegen mogelijke resistentiemechanismen gerichte behandelingen: ceralasertib (ATR kinaseremmer), olaparib (PARP-remmer), danvatirsen (STAT3 antisense oligonucleotide), of oleclumab (anti-CD73). Het primaire eindpunt was objective response rate. De ORR was 13,9% met durvalumab-ceralasertib versus 2,6% met de gepoolde drie andere behandelingen. De figuur laat de progressievrije overleving en overall survival zien. Het veiligheids/tolerabiliteitsprofiel van durvalumab-ceralasertib was manageable.
{kind=link}
De onderzoekers concluderen dat de combinatie van durvalumab en ceralasertib voor immuuntherapie-refractair NSCLC nadere bestudering verdient (fase 3 LATIFY studie; NCT05450692).
1.Besse B, Pons-Tostivint E, Park K et al. Biomarker-directed targeted therapy plus durvalumab in advanced non-small-cell lung cancer: a phase 2 umbrella trial. Nat Med 2024-02808-y
Summary: The multinational phase 2 HUDSON trial found promising activity of the combination of durvalumab and ceralasertib for immunotherapy-refractory advanced non-small lung cancer.